Hyperthemia
fever가 아니다.(fever는 inflammation의 산물이다.)
hyperthemia는 central thermoregulation의 dysfunction이다.
Malignant neuroleptic
syndrome
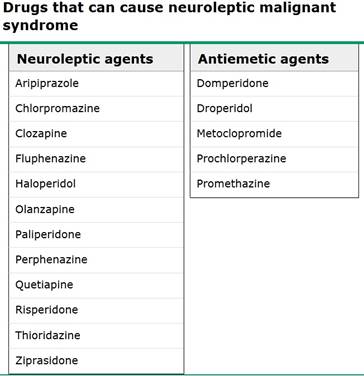
Antipsychotic 약제에 의해 유발됨(dopamine 의 block으로 유발)
typical high potency : halloperidol , Fluphenazine
low potency : CPZ(chlorpromazine)
Atypical agent : clozapine, risperidone
Antiemetics : metoclopromide , promethazine
Pathogenesis : 잘 모른다. 몇가지 가설이 있다.
전형적 증상 : mental change (주로 agitated delirium, confusion), stupur, coma로 진행
extreme muscular rigidity(lead pipe형태 , tremor가 동시에 발생시, cog wheel movement형태가 됨)
hyperthemia
autonomic instablity
1.(가장 유력한 가설) Thalamus 의 dopamine receptor blockade로 인한 thermoregulation의 장애로 인해 hyperthemia 발생, dysautonomia 발생(tachycardia, High BP , tachypnea, dysrhythmia, 다량의 발한)
2. nigrostriatal pathyway의 dopamine blockade로 인한 parkinsonian symptom 발생
-> rigidity, tremor
3. peripheral muscle에 direct toxicity로 작용하여 muscle의 mitochondrial dysfuction
4. sympathetic system의 장애를 일으켜 muscle tone의 증가, HR상승, metabolism 증가, vasomotor sudomotor activity를 억제하여 열발산을 억제함.
dopamine antagonist를 쓰면, dopamine 의 efferent sympathetic regulation의 장애를 일이킨다.
치료 : single most important treatment 원인 약제 끊기
lithium, anticholinergic therapy, serotonergic agents 이런것들도 먹고 있으면 끊기
ICU 입원
DVT 예방위해 heparin 쓰기
Agitation 이 있을때는 benzodiazepine(lorazepam, clonazepam)쓸것
그외 supportive care
입증되지 않은 치료로 Dantrolene, bromocriptine, Amantadine(domaminergic, anticholinergic effect), levodopa등이 있다.
Prognosis
대부분 2주 이내에 회복된다.
mortality rate 10~20%
myoglobinuria, renal failure 발생시 mortality높다.
alcoholics , drug abuse일때 mortality높다.
high potency agent일때 mortality높다.
Neuroleptics의 재시작
재발의 여부는 알수 없다. 환자마다 다르다.
재발을 최소화 하는 guideline(성공을 guarantee하지는 못한다)
1. 최소 2주 기다려라. 될수 있으면 오래
2. lower potency drug 쓰고, low dose로 시작 천천히 titrate해라
3. lithium 동시에 쓰지마라
4. 탈수를 피하라
5. NMS 증상 모니터하라.
Serotonine syndrome
serotonine의 작용
central : attention, behavior , thermoregulation
peripheral : GI motility 증가, vasoconstriction, uterine contraction , bronchoconstriction
GI tract의 enterocromaffin cell에서 분비되어 irritant substance에 반응하여 serotonin분비 하면 diarrhea 발생 , blood 의 serotonin의 level이 올라가면 CNS의 chemoreceptor trigger zone에 작용하여 vomiting을 일으킨다. enterocromaffin cell은 chemotherapy에도 민감하게 반응한다.
증상(SSRI로 인한 serotonine의 증가로 인하여 발생함)
Mental change (anxiety, agitated delirium, restlessness, and disorientation)
Autonomic manifestations ( diaphoresis, tachycardia, hyperthermia, hypertension, vomiting, and diarrhea)
Neuromuscular hyperactivity can manifest as tremor, muscle rigidity, myoclonus(pronounced in the lower extremities), hyperreflexia, and bilateral Babinski sign
진단기준 : SSRI를 먹고 있으면서 하기 증상중 하나를 가질때(hunter criteria)
1. spontaneous clonus
2. Inducible clonus plus agitation or diaphoresis
3. Ocular clonus plus agitation or diaphoresis
4. tremor and hyperreflexia
5. hypertonia
6. temp 38도 초과 plus clonus or inducible clonus
치료
1. 약제 끊기
보통 약제 중단하루만에 좋아지지만, half-life가 긴약물일 경우 최대 2주까지 지속된다.
Ex. fluoxetine : half life : 1주일 , metabolite 2.5주일
MAOI를 쓸경우 몇주정도 지속될수 있다.
2. Agitation 의 management : benzodiazepine 으로 agitation 및 mild HR상승 및, mild BP 상승을 control할 수 있다.(physical restraint는 환자가 isometric muscle contraction을 일으키므로 hyperthemia 및 lactic acidosis를 일으킨다.)
Severe hypertension , tachycardia : esmolol, nitroprusside
MAOI에 의하여 유발된 hypotension은 phenylephrine, epinephrine, norepinephrine 를 쓰자, dopamine(indirect로 epi와 norepi로 변환되어 작용)은 쓰지 마라..
benzodiazepine과 supportive care로 agitation과 autonomic 증상이 해결이 안될때 Cyproheptadine(histamine H1 antagonist, nonspecific 5-HT1A(SEROTONINE) and 5-HT2A antagonistic properties) 12 mg is recommended, followed by 2 mg every two hours until clinical response is seen
3. hyperthrmia 의 management
Fever 가 아니므로 acetaminophen은 효과가 없다. 쓰면 안된다.
IV crystaloid 주입
고열이 발생시 41도 이상시 응급상황대비 (자발호흡 감소시 intubation) , rectal temp측정
38~39도로 떨어지면, cooling stop(iatrogenic hypothrmia 발생 억제위해)
스프레이로 물을 뿌리고, 바람을 불어주는 방법이 효과적임
shivering이 발생시 benzodiazepine을 주입(diazepam, lorazepam)하면, shivering억제 및 약제자체의 약한 체온을 떨어뜨리는 효과가 있음
ICE water 입수방법, ICE pack을 겨드랑이, 목, 사타구니(큰혈관들이 지나가는 길)에 대는 방법등이 있다.
그외 cooled air, cooled blanket, cold IV fluid(섭씨 22도)주입 등의 방법도 있다.
고열의 합병증
· Respiratory dysfunction
· Seizures
· Vomiting and diarrhea
· Rhabdomyolysis
· Acute kidney injury
· Hepatic injury
· Disseminated intravascular coagulation
여기까지 uptodate 19.3